
Diagnostic Safety
Diagnostic Safety
Unfortunately diagnostic errors still happen despite all efforts to improve safety of healthcare systems and figures vary according to the method of measurement and healthcare setting. However, reported figures show that 5%-15% of patients suffer from diagnostic errors, some of grave consequences.
A diagnostic error occurs when a diagnosis is either delayed, wrong, or missed. Failure to communicate a diagnosis to the patient and family/carer is also considered a diagnostic error. Diagnostic errors can occur at any stage of the diagnostic journey and can be challenging to spot as they require definitive information and time for them to be realized.
Contrary to what might be expected, diagnostic errors occur with commonly-encountered health problems such as cancer, cardiovascular problems, stroke, pulmonary embolism, fractures, and infections.
Clinical (Diagnostic) Reasoning
It is suggested that diagnosticians use two modes of thinking, reasoning, and decision making during a diagnostic process. The intuitive approach (system 1) is rapid, subconscious, and effortless. It is used most of the time and depends on pattern recognition based on previous experiences but it is error prone. On the other hand, the analytic approach (system 2) is slow, deliberate, conscious and effortful. It is used when the situation is novel and there is ample time for data collection and analysis. It is considered to be more reliable and less error prone.
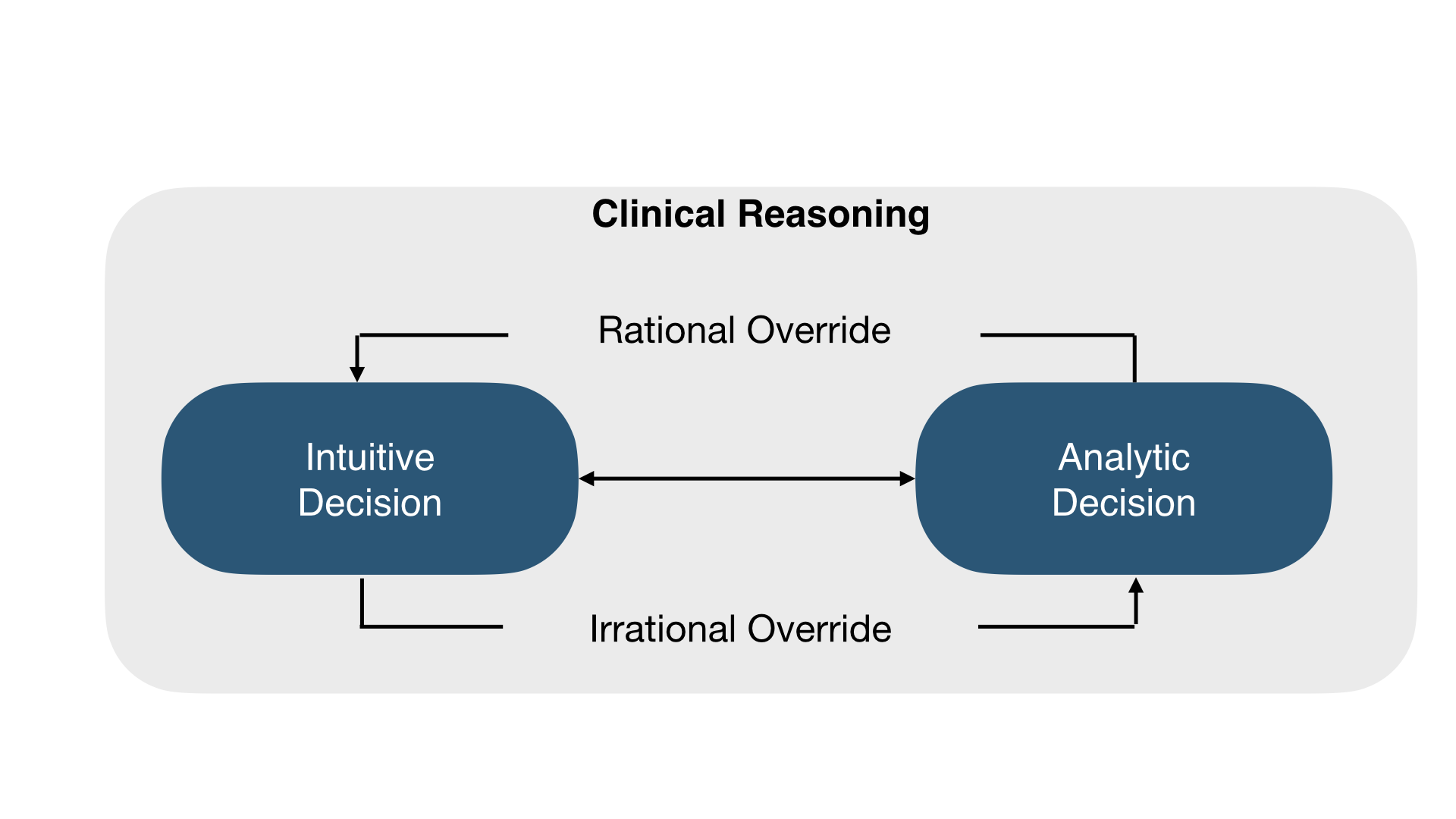
The two systems are not mutually exclusive and we tend to use both modes to reach a final diagnosis through a process of calibration. A rational override occurs when system 2 rejects system 1 while, an irrational override occurs when system 1 rejects system 2.
IPPSEP Diagnostic Framework
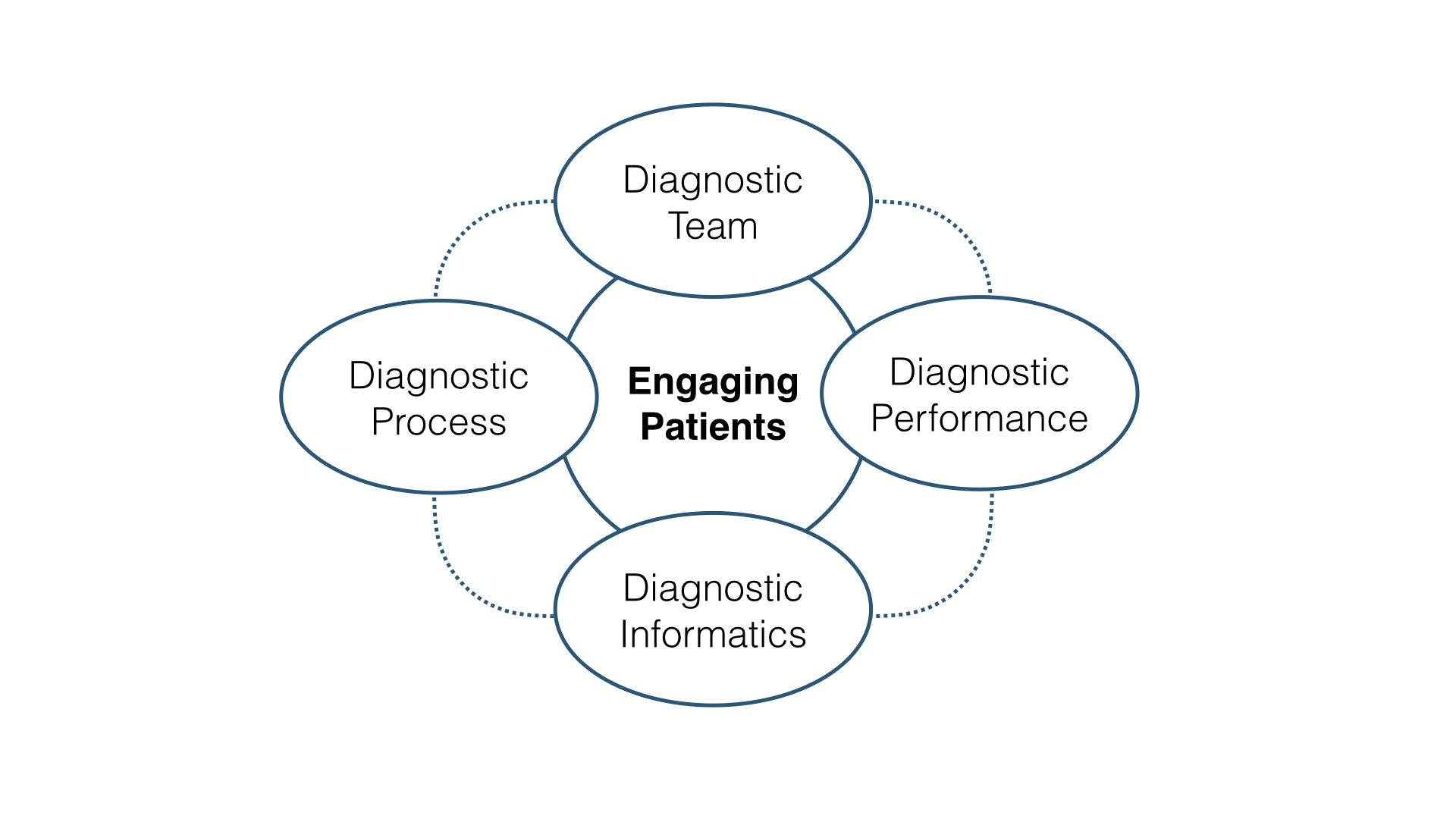
We present diagnostic safety under five essential headings derived from the Health Governance Unit framework for InterProfessional Patient Safety Education and Practice (IPPSEP).
Diagnostic Process
The first step in diagnostic safety is to follow the diagnostic process which is a collaborative cycle of information gathering (patient interview, clinical examination, test ordering, consultation), information integration and interpretation, and determination of a working diagnosis which may be either a list of potential diagnoses (differential diagnosis) or a single potential diagnosis. The list is refined as further information is obtained. As the list becomes narrowed to one or two possibilities, diagnostic refinement of the working diagnosis becomes diagnostic verification.
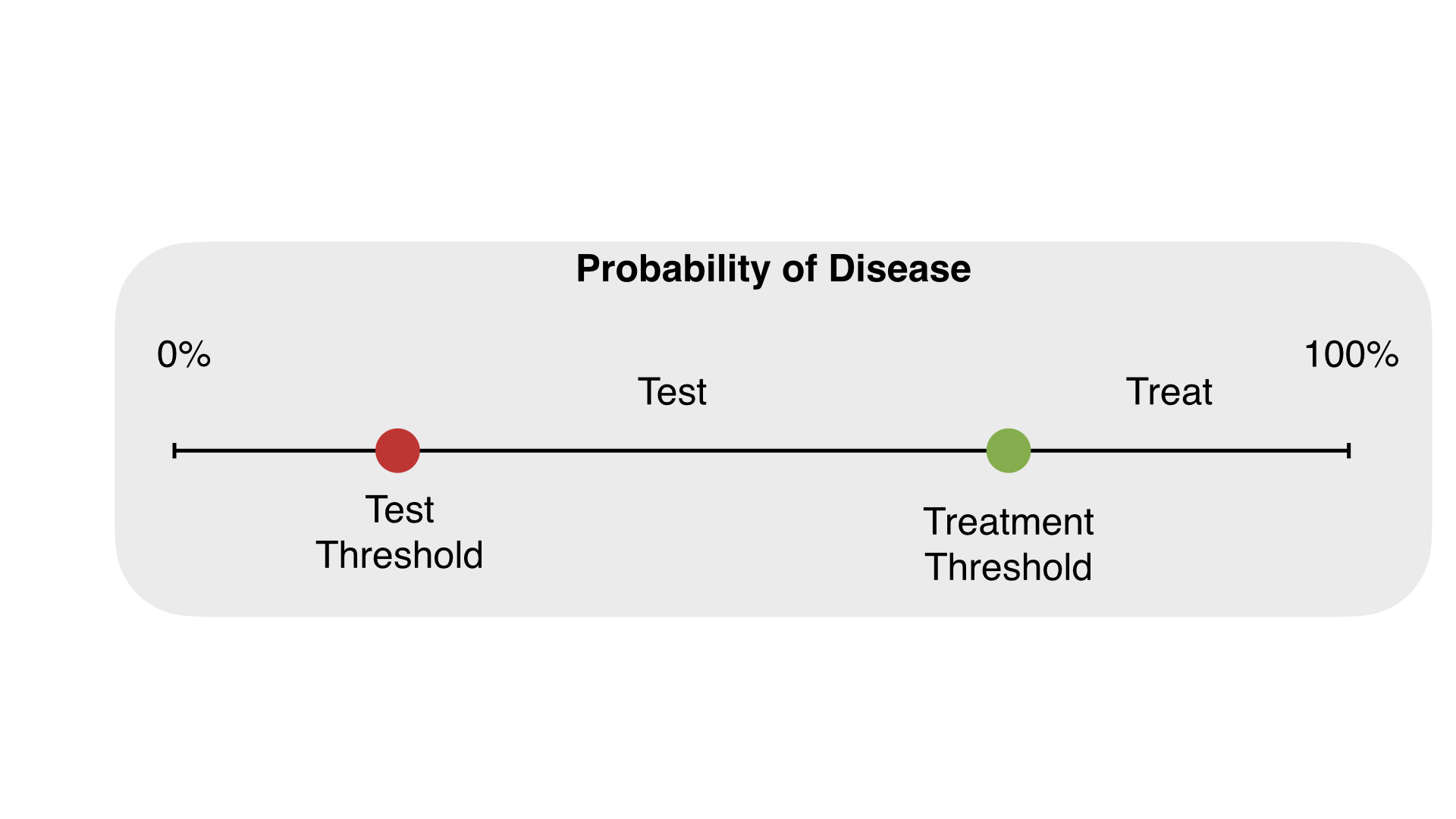
It is important that the diagnostic process in itself does not pose a risk to patient safety by ordering too many invasive diagnostic procedures or by taking so much time that treatment is delayed. Being aware of the test-treatment threshold (below which testing is not warranted and above which treatment is justified) is important and represents a more analytic approach to clinical decision-making.
Diagnostic Teams
Diagnosis is a teamwork process involving a group of diagnosticians and other healthcare professionals who support the diagnostic process. Diagnosticians are professionals who have been educated and licensed to provide patients with diagnosis such as physicians, pathologists, radiologists, and certain assistants who have been trained in the diagnostic process. Diagnostic teams are dynamic as their membership varies depending on the patient’s health problem and what expertise is needed to reach an accurate diagnosis. Effective diagnostic teams have a common goal, agreed upon roles and responsibilities, meet regularly, respect each other, and work through data and information.
Engaging Patients
The working diagnosis of the patient health problem should be shared with the patient, including the degree of uncertainty associated with it. Each time there is a revision of the working diagnosis, this information should be communicated to the patient. Patients should be considered active members of their diagnostic teams as they are most aware of their health journey and can facilitate communication and decisions among team members. However, patients may be reluctant to engage and so providers should make them feel safe to speak and express their views. Patients can be empowered through access to their medical records and relevant diagnostic information.
Diagnostic Informatics
Healthcare facilities should make sure that their diagnostic teams have access to current diagnostic criteria, algorithms and checklists of the common health problems they encounter to ensure evidence-based diagnostic decisions. Data and information on diagnostic errors and related harm at each step of the diagnostic process should be collected and analyzed to create and share the necessary knowledge and wisdom to minimize their occurrence. Assessment of patient engagement and teamwork within and among diagnostic teams should be performed and its results made available to all.
Diagnostic Performance
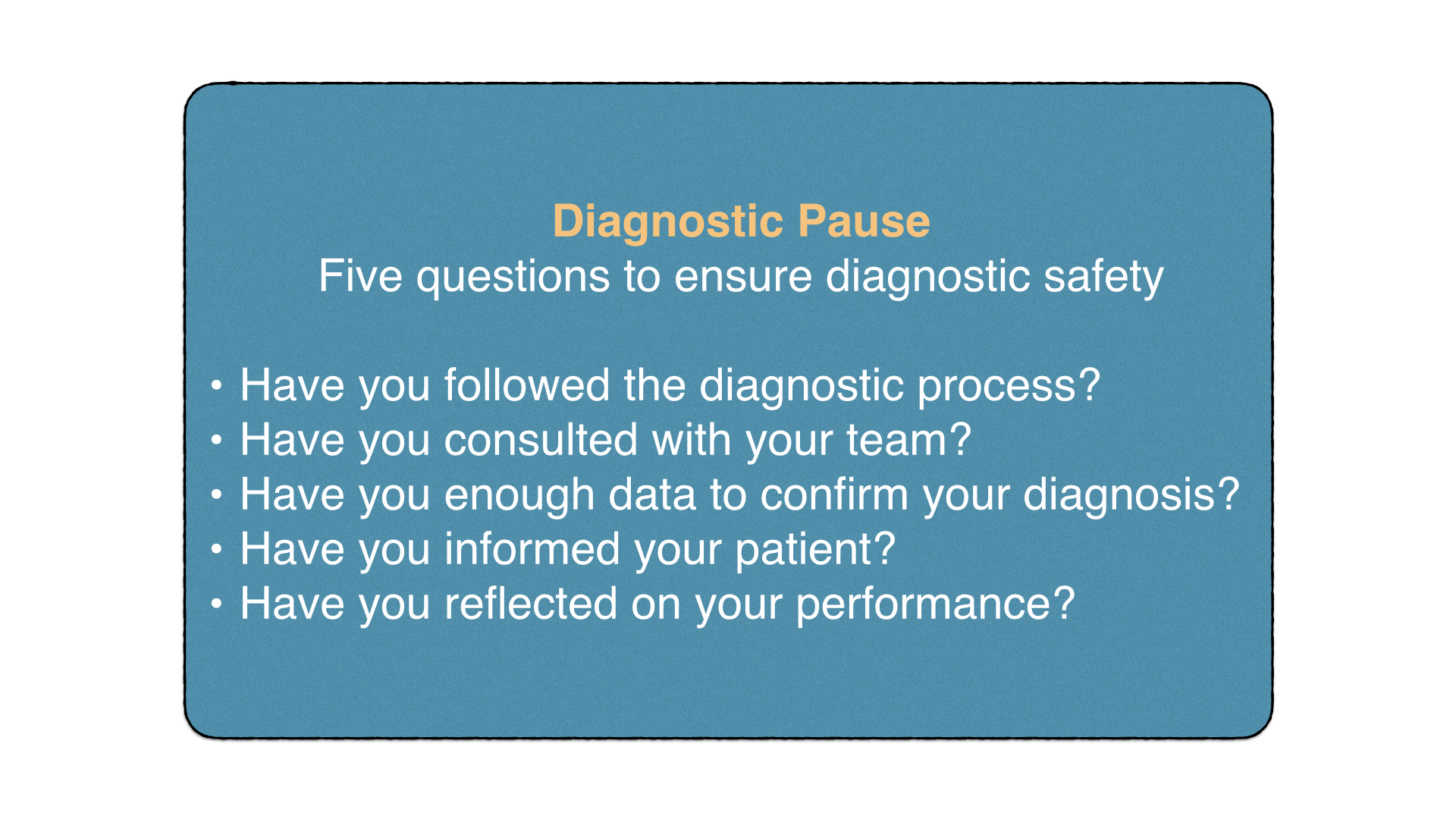
Healthcare providers should work towards improving their diagnostic performance as part of their commitment to improve patient safety. There are many tools that can be utilized to improve diagnostic performance such as mnemonics, checklists, and decision aids. We present below a simple generic tool, Diagnostic Pause, that healthcare providers can utilize to reflect on their performance in the five main areas that are critical to diagnostic safety.
Reading Material
-
- Diagnostic errors. Technical series on safer primary care. WHO. 2016.
- Improving diagnosis in health care. NASEM. 2015.
- Crosskerry P. A universal model of diagnostic reasoning. Acad Med. 2009;84:1022-8.
 8- ABC of PS - DS-.pdf
8- ABC of PS - DS-.pdf